
Any musculoskeletal alteration comes along with postural patterns compensations that seem to be constant and are very well defined in humans according to Myers T (ix) but not as well described in horses. Elbrond & Shultz (2014) describes Myofascial Kinetic Lines in horses. Below you can find a detailed comparison of the backline on equines based on a level III of scientific evidence.
Superficial ventral line:
This chain generates rapid movements so there is a higher percentage of type II fibers and it begins at the anterior base of the third phalanx and connects the entire anterior aspect of the hind limbs, the entire ventral aspect of the abdomen and the neck, ending on both lateral parts of the skull.
- Its postural function is to balance the superficial dorsal line and in order to achieve it the occiput must be taken as a fixed point, providing elastic / contractile support to the thorax, abdomen and pelvis.
- Its movement function is the global flexion of the body but on the stifles and occipital-atlas-axis joint it provides extension.
Specifically, postural patterns compensation when this line is altered appear to be:
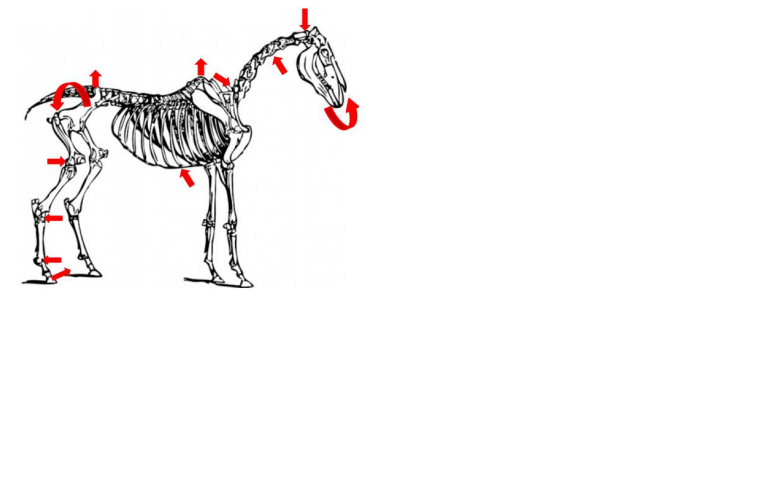
- Tendency to horizontalization of the third phalanx. The tendon of the extensor digitorum longus can be found in a short position and the tendon of the flexor digitalis longus muscle in a long position.
- Tendency to hyperextension of the fetlock producing a limitation of the flexion in the fetlock.
- Tendency to flex the hock due to possible short position of the common digital extensor muscle. The deep digital flexor muscle and the gastrocnemius muscle can be found in a long position.
- Tendency to flex the stifle. The semitendinosus and biceps femoris muscles may be in a short position and the semimembranosus and quadriceps femoris muscles are in a long position.
- Posterior pelvic tilt or pelvic retroversion due to possible short position of the psoas minor muscle, the gluteus superficial and tensor fascia lata muscles. The gluteus medius, gluteus medius, and piriformis muscles may be in a long position.
- Tendency to contranutation of the sacrum. The short position of the pelvic muscles produces this alteration.
- Tendency to lumbar kyphosis / correction due to possible short position of the abdominal muscles.
- Increased kyphosis of the withers due to possible short position of the abdominal muscles.
- Posterior inclination of the thoracic cage due to the possible blockage in short position of the caudal serratus dorsalis, the internal intercostal muscles and the transverse thorax muscle. The cranial serratus dorsi muscles, external intercostals, ribs elevators, and rectus abdominal may be in a long position.
- Tendency to decrease low cervical lordosis as the long neck muscle and the sternomandibular muscle may be in a short position. The cervical iliocostal muscles, the longus muscle of the neck, and the multifidus muscle in its cervical portion may appear in a long position.
- Tendency to increase upper cervical kyphosis and flexion of the occipital-atlas-axis complex. The short position of the long muscle of the head, the lateral and ventral rectus muscles of the head as well as the cleidomastoid and sternomandibular muscles can produce this alteration. In addition, it is possible to see a tendency to posterior translation of the head and a posterior sliding of the occiput with respect to the atlas.
ix Thomas W. Myers